CIMERLI® resources for you and your patients
Information to support you, your patients, and your practice.
For healthcare providers
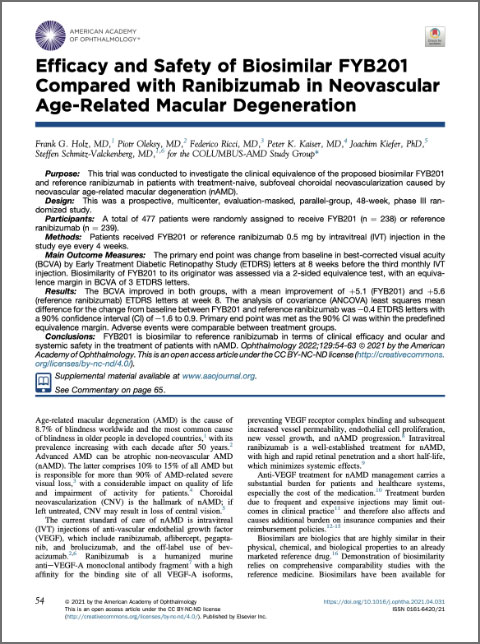
The COLUMBUS-AMD Study
The COLUMBUS-AMD Study was an equivalence trial of CIMERLI® and reference product Lucentis® (ranibizumab injection) in patients with wAMD.1
Review the COLUMBUS-AMD Publication (opens in a new tab)Download the COLUMBUS-AMD Presentation (opens in a new tab)
Sandoz One Source®
for CIMERLI®
Sandoz One Source provides comprehensive practice and patient support.
See the Payer Coverage CenterDownload the Brochure (opens in a new tab)For your patients

CIMERLI® Patient Brochure
The patient brochure includes information about CIMERLI®, biosimilars, and the financial support that may be available to your patients.
Download the Brochure (opens in a new tab)For practices
Download All (opens in a new tab)Product Ordering Form
Download Product Ordering Form (opens in a new tab)Sandoz One Source Enrollment Form
Download Sandoz One Source Enrollment Form (opens in a new tab)Sandoz One Source HCP Portal User Guide
Download User Guide (opens in a new tab)CIMERLI® Coding Flashcard
Download Coding Flashcard (opens in a new tab)Sample Coding Sheet (CMS 1500 Form for Outpatient Claims)
Download CMS 1500 Form (opens in a new tab)Sample Coding Sheet (CMS 1450 Form for Hospital Inpatient Claims)
Download CMS 1450 Form (opens in a new tab)Comprehensive Billing & Coding Guide
Download Billing & Coding Fact Sheet (opens in a new tab)Product Fact Sheet
Download Product Fact Sheet (opens in a new tab)Letter of Medical Necessity
Download Letter of Medical Necessity (opens in a new tab)Letter of Appeals
Download Letter of Appeals Form (opens in a new tab)Product Replacement Request Form
Download Product Replacement Request Form (opens in a new tab)Co-pay Program Virtual Debit Card Request
Download Virtual Debit Card Fax Request (opens in a new tab)Co-pay Program Operations Guide
Download Co-pay Program Operations Guide (opens in a new tab)Sandoz One Source provides comprehensive practice and patient support
Discover Sandoz One Source SupportRequest a visit from a Sandoz representative
Connect With Us